

LEARNING OBJECTIVES
1-Introduction
2-Definition
3-Causes of esophageal varices
4-Pathophysiology
5- Clinical features
6- Classification of esophageal varices
7- Diagnosis
8- Management of esophageal varices
9- Complications
10- Prognosis
11- Conclusion
12- Quiz
INTRODUCTION:
Esophageal varices are enlarged abnormally dilated veins which mostly occur in lower 3rd part of esophagus due to high pressure in portal vein[portal hypertension].They are dangerous because they can rupture and cause bleeding.
DEFINITION:
Dilated tortuous veins in the esophagus as a result of portal hypertension commonly due to liver cirrhosis
OTHER SITES:
Can develop in other sites
- Gastric varices[found in stomach]
- Rectal varices[swollen veins in rectum mostly known as hemorrhoids]
- Caput medusae[enlarged veins appearing on abdomen radiating from navel]
- Duodenal varices[enlarged veins in duodenum-first part of small intestine]
*CAUSES OF ESOPHAGEAL VARICES
1-PRE-HEPATIC CAUSE
- Portal vein thrombosis[blood clot in portal vein which carries blood from digestive system to liver]
- Portal vein obstruction[it occur when blood flow to liver is blocked or slowed down]
- Splenic vein thrombosis[clot in vein draining spleen]
- Splenomegaly[enlargement of spleen]
2-HEPATIC CAUSES
- Schistosomiasis[parasitic infection caused by blood fluke -flat worms. The parasite lodge its egg in portal vein causing inflammation and fibrosis. This blocks blood flow in liver . ]
- Congenital hepatic fibrosis[rare inherited condition in which liver develops malformed bile duct and fibrous tissue]
- Idiopathic[unknown cause]
3-POST HEPATIC CAUSES
- Budd-Chiari syndrome[hepatic vein draining blood away from liver to hear are blocked due to blood clot]
- Right sided heart failure[ right side of heart fails to pump blood to lungs and blood will backflow to systemic circulation via inferior vena cava

CLINICAL FEATURES OF ESOPHAGEAL VARICES:
SYMPTOMS:
- Early asymptomatic
- Fatigue
- Loss of appetite
- Weight loss
- Hematemesis[blood in vomiting]
- Melena [black color stools]
SIGNS
- Hypotension[low blood pressure]
- Tachycardia[fast heart rate]
- Pale skin
- Ascites[fluid in abdomen]
- Jaundice
*DIAGNOSIS OF ESOPHAGEAL VARICES:
1-History
vomiting
black stools
jaundice
Ascites
3-LABORATORY INVESTIGATION
- CBC=Anemia ;low platelets
- LFTs =Abnormal
- PT\INR=Prolonged
4-IMAGING STUDIES
- Ultrasound abdomen
- CT-scan\MRI
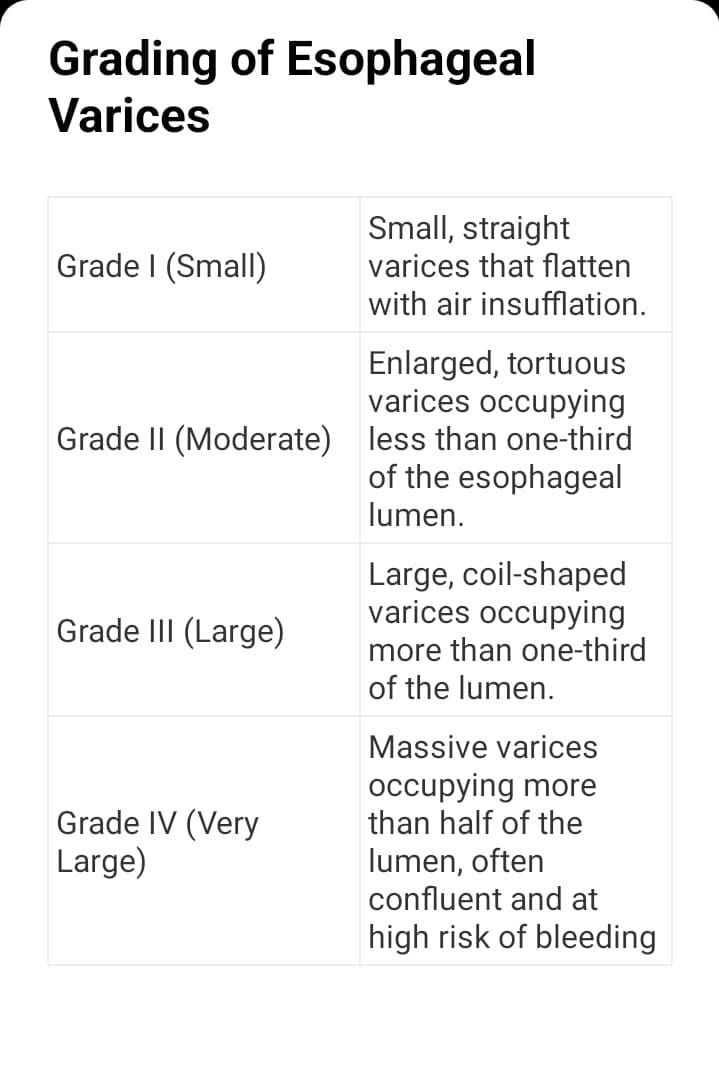
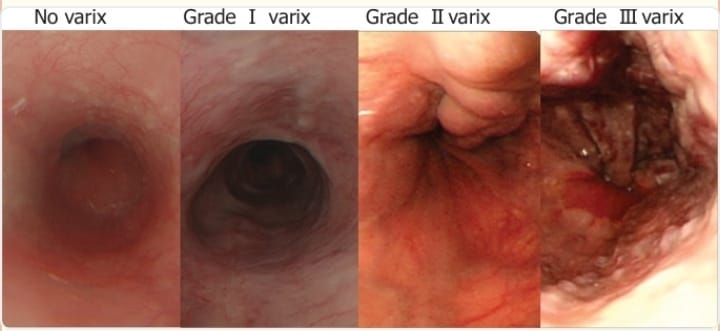
Grading of Esophageal Varices
Esophageal varices are graded endoscopically according to their size.
BAVENO GUIDELINES
Many current guidelines classify varices simply as:
- Small varices
- Large varices >5mm
High Risk Endoscopic Signs
- Red whale marks
- Cherry red spots
- Hematocystic spots
MANAGEMENT OF ESOPHAGEAL VARICES:
- Work up and treatment of portal hypertension
- Airway stabilization
- Resuscitation fluid=maintain Hb up to 7g\dl
- Vasoactive drugs=
- Terlipressin (first-line in many guidelines)
- Octreotide
- Somatostatin
- Endoscopic treatment=band ligation[Sclerotherapy]
- Balloon tamponade
Treatment of Esophageal Varices
- Acute bleeding
- Primary prophylaxis
- Secondary prophylaxis
Management of Acute bleeding:
- i- Airway breathing and circulation control
- ii- IV fluids
- iii- blood transfusion
- Vasoactive drugs {Octreotide, Terlipressin}
- iv- Antibiotics{ Ceftriaxone} to prevent infection in cirrhosis patient
- v- Urgent endoscopy
- vi- EVBL ( in this process a rubber band is placed around the dilated when to stop bleeding)
- vii- Sclerotherapy ( in this process sclerosant injection is administered into the dilated when which stops the bleeding)
- viii- Balloon tamponade (in this process a balloon is dilated to apply pressure on dilated when ever the pressure is applied that dilated veins compresses and it stops blood ultimately.)
- ix- TIPS (it is a radiological process in which a channel is created between portal vein and hepatic vein to reduce portal hypertension and bleeding varices. It allows blood to bypass hepatic vein and flow directly to systemic circulation.)
2- Primary prophylaxis:
It is prevention of first bleeding or prevention of bleeding in future when patient already know about varices .
i- Beta blocker PropranololCarvedilol
ii- EVBL
.jpeg)

3- Secondary prophylaxis:
It is prevention of recurrent bleeding from varices.
i- Combination of Beta blocker
ii- Repeat EVBL
iii- Treat the cause (hepatitis, cirrhosis)
Emergency warning🚨🚑
- Blood in vomiting 🩸
- Black color stool⚫
- Fainting 😵💫
- Low blood pressure 🪫
- Confusion🫤
*COMPLICATION:
- HEMATEMESIS
- MELENA
- HYPOVOLEMIC SHOCK
- ANEMIA
- ASPIRATION PNEUMONIA
- HEPATIC ENCEPHALOPATHY
- INFECTION
- STRICTURE
- ULCERATION
*PROGNOSIS:
Esophageal varices are asymptomatic early. Their Prognosis is poor if bleeding occurs .Prognosis is better if varices are detected early and prevented from bleeding
*SUMMARY:
Esophageal varices results from portal hypertension
Screening is very important
Upper GI endoscopy is good for diagnosis
Long term prevention include betablocker and band ligation
FAQs:
1-What is most common cause of esophageal varices?
2-Name gold standard test for esophageal varices?
3-How many grades of esophageal varices are in above classification?
ANSWERS: 1-Portal hypertension 2-Upper GI endoscopy 3-there are 4 grades of esophageal varices.
References
- Sleisenger and Fordtran’s Gastrointestinal and Liver Disease. Feldman M, Friedman LS, Brandt LJ, editors. 11th ed. Philadelphia: Elsevier; 2021.
- Sherlock’s Diseases of the Liver and Biliary System. Dooley JS, Lok ASF, Garcia-Tsao G, Pinzani M, editors. Wiley-Blackwell; 2022.
- American Association for the Study of Liver Diseases (AASLD). Practice guidance on portal hypertension and variceal bleeding.
- European Association for the Study of the Liver (EASL). Clinical Practice Guidelines on the management of portal hypertension.
- Baveno VII Consensus Workshop. Renewing consensus in portal hypertension. Journal of Hepatology. 2022.
- American Society for Gastrointestinal Endoscopy (ASGE). Guidelines on the role of endoscopy in the management of variceal hemorrhage.
- Robbins and Cotran Pathologic Basis of Disease. Kumar V, Abbas AK, Aster JC. Elsevier; 2020.