
")
Introduction
Gastritis is the inflammation of the gastric (stomach) mucosa. In long-standing cases, this inflammation damages the stomach lining, leading to erosions, ulcers, bleeding, atrophy, or malignancy.
It occurs when an imbalance develops between the protective mechanisms of the stomach and damaging factors:
Gastritis is not a single, uniform disease but a spectrum of conditions. The cause, pathological changes, and clinical behavior vary widely. It is classified into different types based on factors such as duration, cause, histological pattern, and endoscopic appearance.
This classification helps in understanding the underlying mechanism, guiding appropriate treatment, and assessing prognosis (especially regarding complications like ulcer formation and gastric malignancy).
1. Based on Duration
Acute Gastritis
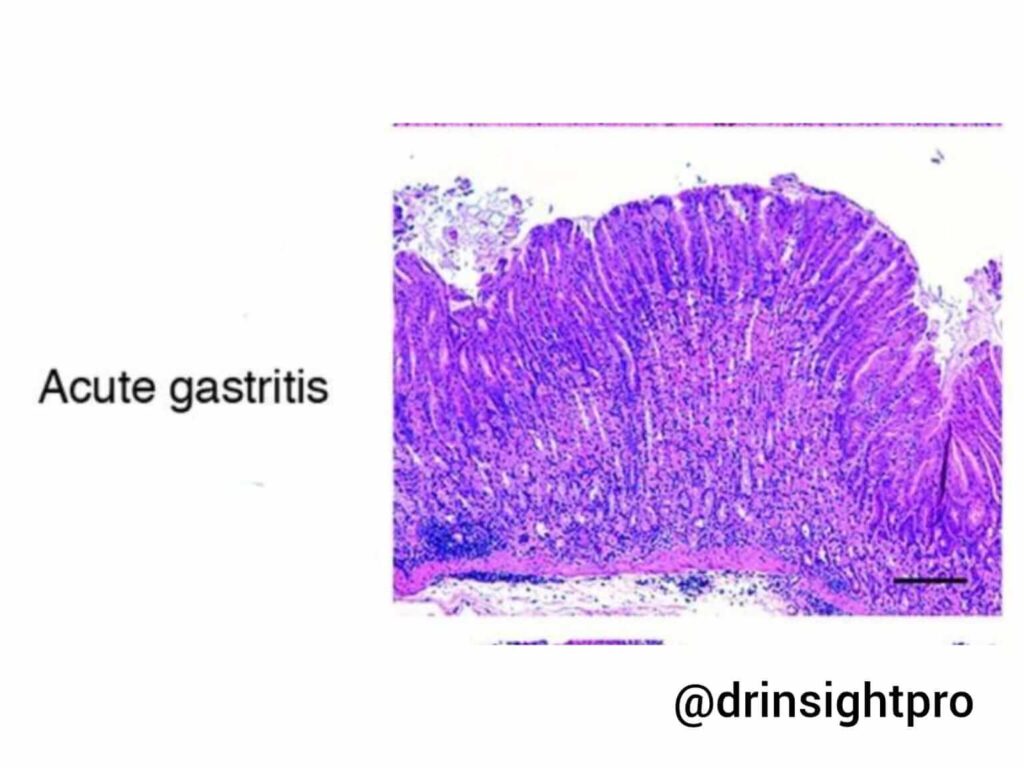
A sudden inflammation of the gastric mucosa characterized by a rapid onset of mucosal injury, which may be mild or severe. It is usually a reversible condition if the cause is removed early.
- Morphology / Endoscopic Findings:
- Diffuse or patchy erythema (redness)
- Edematous (inflamed) mucosa
- Multiple erosions (superficial breaks in the mucosa)
- Petechial hemorrhage (small, pinpoint marks that appear on the mucosa due to bleeding from capillaries)
- Histopathology:
- Neutrophilic infiltration
- Surface epithelial damage
- Edema of lamina propria
- In severe cases: Mucosal necrosis and hemorrhage
Chronic Gastritis
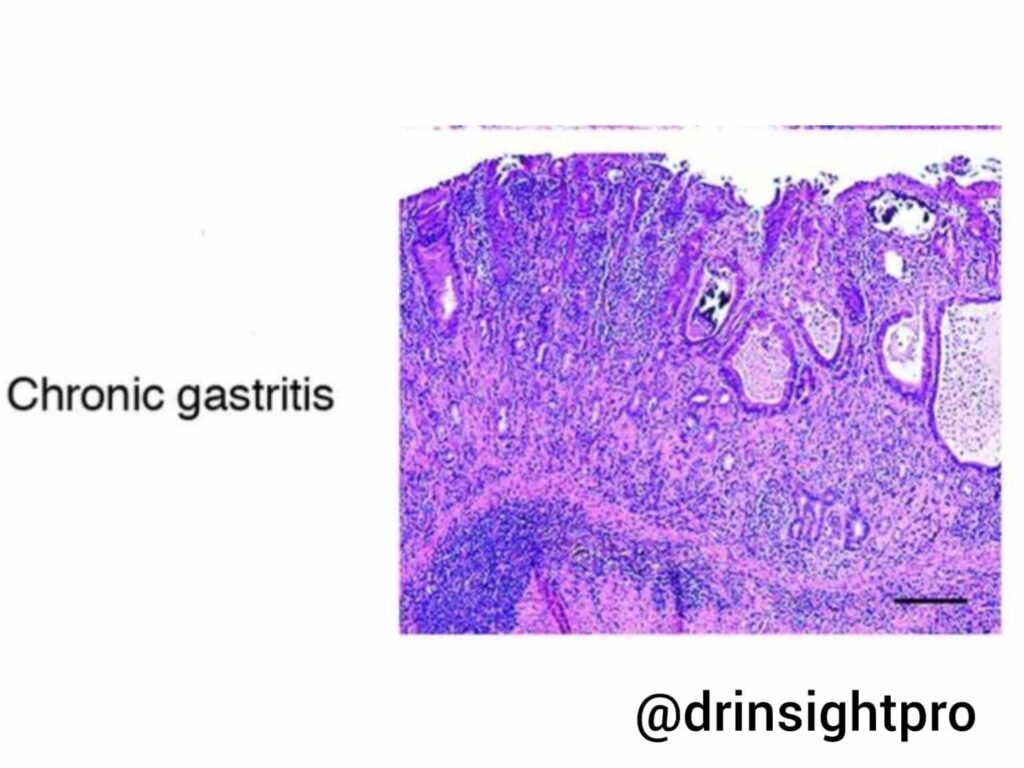
A long-standing inflammation of the gastric mucosa that develops slowly over time and may remain for months to years. It is most commonly caused by infections like H. pylori or the autoimmune destruction of gastric parietal cells.
| Feature | Type A Gastritis (Autoimmune) | Type B Gastritis (H. pylori) | Type C Gastritis (Chemical/Reactive) |
| Definition | Autoimmune destruction of parietal cells and intrinsic factor; associated with antibodies against gastric mucosa. | Caused by an infection with H. pylori. | Chemical injury caused by agents like NSAIDs, alcohol, or bile reflux. |
| Common Site | Mostly seen in the gastric body and fundus (corpus). | Mostly seen in the antrum of the stomach; may progress to pangastritis. | Usually occurs in the antrum or is diffuse. |
| Endoscopic Features | • Pale, thin mucosa • Loss of folds • Visible blood vessels | • Diffuse erythema • Nodular gastritis • Erosions | • Hyperemia (red mucosa) • Minimal inflammation |
| Histology | (See general chronic features below) | (See general chronic features below) | • Foveolar hyperplasia • Edema • Minimal inflammatory cells (Key Point) |
| Clinical Features | Symptoms of Vitamin B12 deficiency (anemia, neuropathy, glossitis/swelling of tongue). | Standard gastritis symptoms. | Standard gastritis symptoms. |
| Complications | • Pernicious anemia • Gastric adenocarcinoma • Gastric carcinoid tumor (ECL cell hyperplasia) | • Peptic ulcers • Gastric adenocarcinoma • MALT lymphoma | Standard progression risks. |
2. Based on Endoscopic Appearance
- Erosive Gastritis: Features erosions (superficial mucosal breaks).
- Non-Erosive Gastritis: No visible mucosal breaks; only edema will be present.
3. Based on Etiology
- Infection: H. pylori
- Drug-Induced: NSAIDs, Aspirin
- Autoimmune: Parietal cell destruction and Vitamin B12 deficiency
- Chemical/Reactive: Bile reflux and alcohol
- Stress-Related: ICU patients, burns, trauma
4. Based on Histology
- Acute Gastritis: Neutrophils are high.
- Chronic Gastritis: Lymphocytes and plasma cells are high; gland atrophy is present.
5. Based on Topography / Location
- Antral Gastritis: Usually H. pylori related.
- Pangastritis: Involves the entire stomach.
- Body / Fundus Predominant: Autoimmune gastritis.
Staging Systems
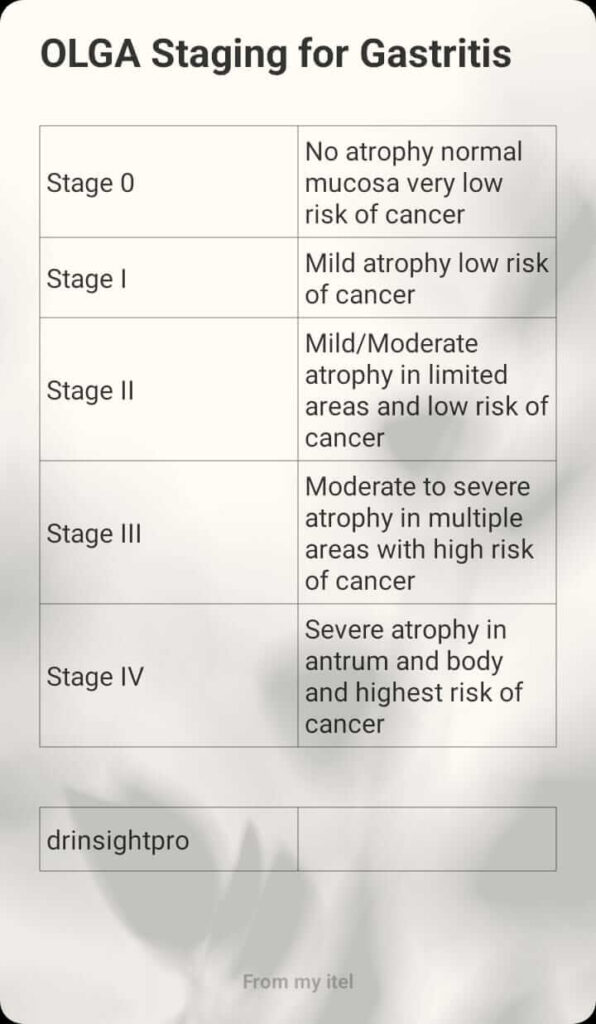
OLGA System (Operative Link on Gastritis Assessment)
The OLGA system is a histology-based system that stages gastritis according to the degree of atrophy and its location (antrum/body). Atrophy is the key parameter because it correlates directly with the risk of gastric cancer.
- Step 1: Biopsy MappingBiopsies are taken from the antrum and body. Each site is graded for atrophy severity:
0= None1= Mild2= Moderate3= Severe
- Step 2: OLGA Stages
- Stage 0: No atrophy, normal mucosa, very low risk of cancer.
- Stage I: Mild atrophy with low risk of cancer.
- Stage II: Mild atrophy with mild to moderate risk of cancer.
- Stage III: Moderate to severe atrophy in multiple sites with a high risk of cancer.
- Stage IV: Severe atrophy in both the antrum and body; carries the highest risk of cancer.
- Clinical Importance: Primarily used to predict gastric cancer risk.
OLGIM Staging (Operative Link on Gastric Intestinal Metaplasia Assessment)
OLGIM is a histopathological staging system used to assess the extent and severity of intestinal metaplasia (IM) in the stomach, especially in patients with chronic gastritis. It is similar to OLGA but focuses on intestinal metaplasia instead of atrophy.
- Why OLGIM is Used:
- Intestinal metaplasia is a more reproducible and stable marker than atrophy.
- It offers better inter-observer agreement than OLGA.
- It helps identify patients at risk of gastric adenocarcinoma.
- Biopsy Protocol: Same mapping protocol as OLGA.
- Grading and Staging of Intestinal Metaplasia:
0= No IM1= Mild focal IM (in the antrum)2= Moderate IM (in limited areas)3= Severe IM (in the antrum or body)- Stage IV: Occurs in both the antrum and body.
- Clinical Importance: Stage III to IV requires endoscopic surveillance, as it is strongly associated with progression to dysplasia and gastric adenocarcinoma.
Clinical Features
Symptoms
- Epigastric pain
- Nausea and vomiting
- Bloating and indigestion
- Early satiety
- Loss of appetite
- Severe Cases: Hematemesis (vomiting blood), melena (black stools), and fatigue (if anemia develops).
Signs
- Epigastric tenderness
- Pallor (indicative of chronic bleeding)
Diagnosis & Management
Diagnosis
- Laboratory Tests:c
- CBC: To check for anemia.
- Serum B12: Evaluated for the autoimmune type.
- Stool Occult Blood: To detect hidden bleeding.
- Tests for H. pylori:
- Urea breath test
- Stool antigen test
- Biopsy urease test
- Upper GI Endoscopy (Gold Standard):
- Visualizes erythema, edema, erosions, bleeding, and atrophy.
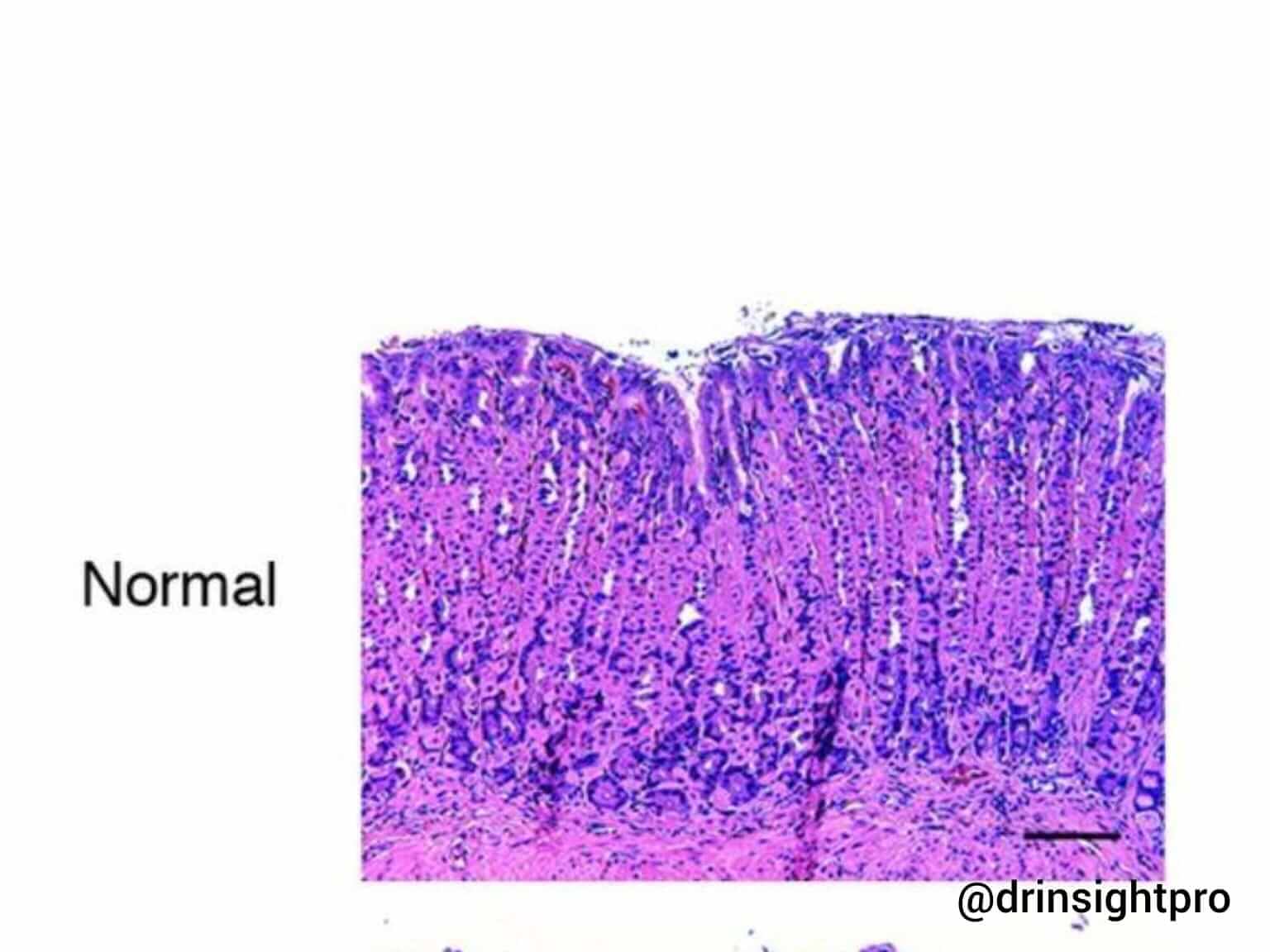
- Histopathology:
- Neutrophils: Indicate acute gastritis.
- Lymphocytes and Plasma Cells: Indicate chronic gastritis.
- May also identify atrophy and intestinal metaplasia.
Management
- General Measures:
- Stop NSAIDs if possible.
- Avoid smoking and alcohol.
- Eat small, frequent meals.
- Medical Treatment:
- Acid Suppression: Proton Pump Inhibitors / PPIs (e.g., omeprazole), beta-blockers.
- If H. pylori Positive: Eradication therapy using a PPI + antibiotics (according to local protocol).
- Autoimmune Gastritis: Vitamin B12 replacements.
- Severe Bleeding: Handled via endoscopic management.
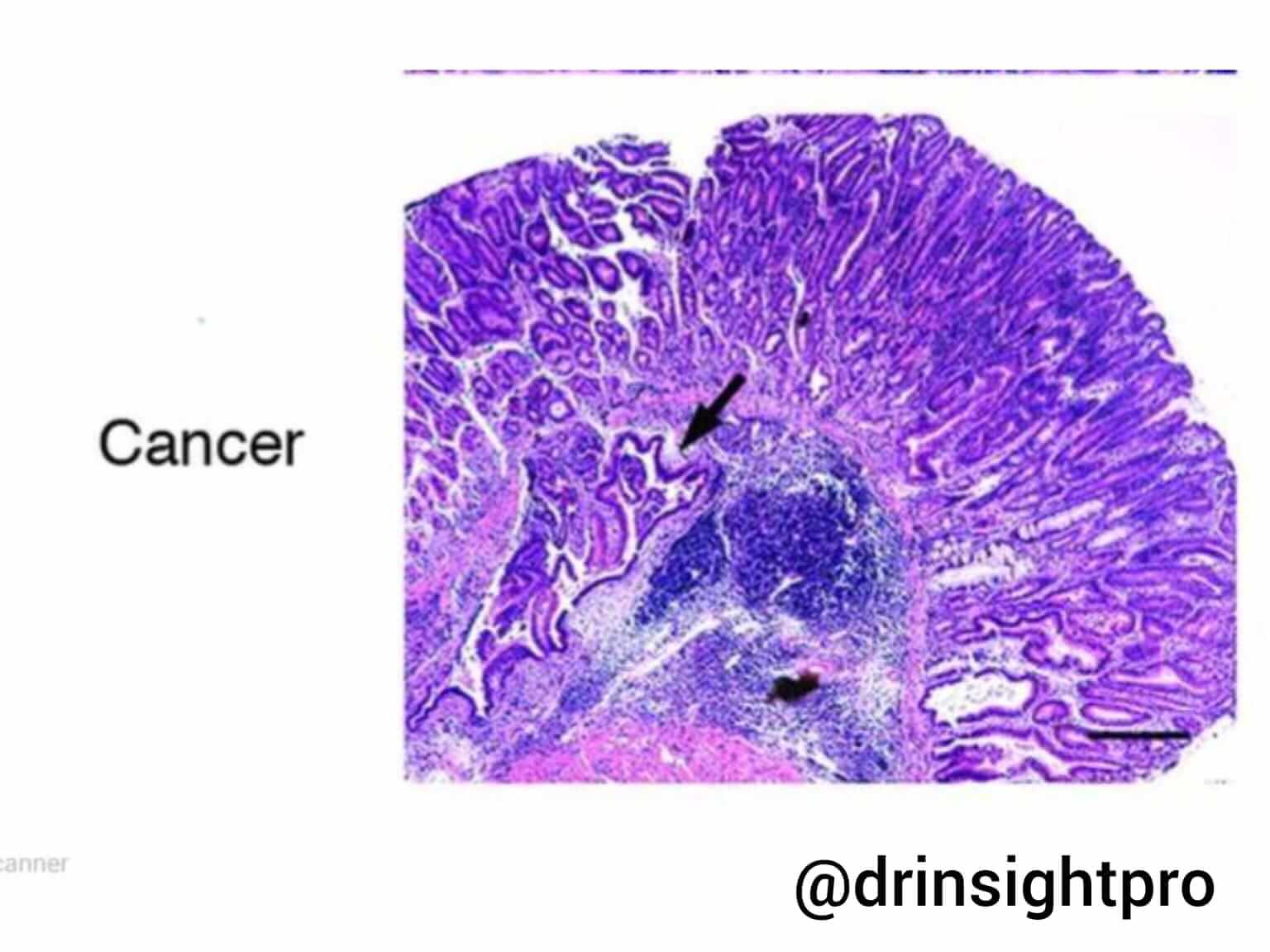
Complications
- Peptic ulcer disease
- GI bleeding
- Iron deficiency anemia
- Pernicious anemia
- Gastric atrophy
- Increased gastric cancer risk
Quiz
Question 1: What are the types of chronic gastritis?
Answer: Chronic gastritis is classified into three main types based on cause, location, and histology:
- Type A (Autoimmune): Destroys parietal cells and intrinsic factor in the gastric body and fundus; leads to Vitamin B12 deficiency and risks pernicious anemia or carcinoid tumors.
- Type B (H. pylori): Mostly affects the antrum; features nodular mucosa and carries a risk of peptic ulcers, adenocarcinoma, or MALT lymphoma.
- Type C (Chemical/Reactive): Caused by chemical irritants like NSAIDs or bile reflux in the antrum; characteristically shows foveolar hyperplasia and minimal inflammatory cells.
Question 2: How do you manage gastritis?
Answer: Gastritis management involves a combination of lifestyle adjustments and targeted medical therapies:
- General: Stop NSAIDs, avoid alcohol and smoking, and eat smaller, more frequent meals.
- Acid Suppression: Use PPIs like omeprazole and beta-blockers.
- Infection Control: Run a combination of a PPI and antibiotics if H. pylori is positive.
- Special Cases: Provide Vitamin B12 replacement for autoimmune gastritis and utilize active endoscopic intervention to manage severe GI bleeding.